|
Spina Bifida and Physical Activity
By, Bernard Baroudi, Undergraduate Student, College of Health and Human Performance, University of Florida, Gainesville, FL
Every year thousands of babies are
born with birth defects that place them
in a predisposition.
This predisposition affects each child
at more than just the physical level.
Birth defects also pierce the psychological
and emotional well-being of each child.
Birth defects range in a wide variety
of forms. Genetic and inherited disorders
are both central issues of concern to
many expecting mothers; however neural
tube defects are the most prevalent
birth defects parents are dealing with
in the United States. This paper focuses
on a disorder often associated with
the term neural
tube defect; spina bifida. Spina
bifida is an occurrence that when in
its most severe form can cause paralysis,
intellectual disability, and other medical
related problems. This condition forms
when the spinal cord and its coverings
are exposed in a newborn's back, occurring
as a result of deficient development
(Complete Home
Medical Guide, 2004). People
dealing with spina bifida deal with
a scope of challenges in everyday routine
living. Through confidence and physical
fitness these people are able to succeed
in every aspect of life. Thanks to adapted
physical exercise, people are able to
fill in the mental and emotional gaps
with which their predisposition has
left them.
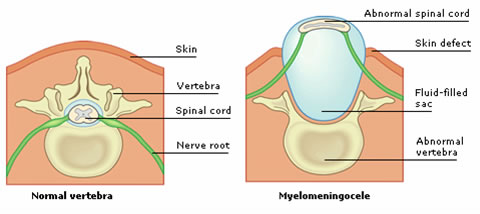
Figure 1. An illustration myelomeningocele, the most severe form of spina bifida.
Spina bifida affects a range of people
unfathomable to those who are not familiar
with the defect. The statistics are
astonishing. According to the AANS (American
Association of Neurological Surgeons),
approximately 70,000 Americans are living
with spina bifida, and now about one
out of every 1,000 births is a neural
tube defect (Science
Letter, 2006). The interesting
thing about Spina Bifida is that it
is not often expected. If your grandfather,
father, and uncles have a history of
chronic heart disease, for example,
then there is a good chance that you
should start your day off with a jog
and forget that the words 'pizza' and
'french fries' exist. However, 95 percent
of children with spina bifida are born
to parents with no history of the disease
(Science Letter,
2006).
Since the arrival of Spina bifida can
rarely be expected, prevention is critical.
Folic acid intake is possibly the best
way to protect your child from any type
of birth defect. However, a fine line
about folic acid is that it should be
taken well before conception to be fully
effective, not when pregnancy has already
been determined. Another step to be
taken is the use of ultrasound early
and frequently. In the occasion that
spina bifida is detected during ultrasound,
immediate surgery can be performed.
In a recent article by Newsome (2007),
a new surgery is highlighted that allows
fetuses with spina bifida an escape
route from permanent disability. Up
until now, it has been common for spina
bifida babies to undergo surgery immediately
after being born to fix the defect and
prevent any more damage from occurring,
however, paralysis and loss of bladder
control may have taken place at this
point. This new type of surgery operates
on the baby while still inside the mother.
The reasoning is that most of the damage
done by spina bifida occurs as the fetus
develops in the womb. Fixing this problem
while the fetus is still developing
may avert any major damage from occurring
(Newsome, 2007).
Another critical facet of spina bifida
is its partnership with hydrocephalus.
It is a condition where unwanted fluid
in the head creates damaging pressure
on the brain. It is a condition familiar
with neural tube defects because it
is apparent in 80 to 90 percent of spina
bifida patients. Hydrocephalus does
not necessarily contribute to the physical
aspect of spina bifida, but does require
a shunt that is prone to surgical revision
every couple of years (Complete
Home Medical Guide,2004).
Since spina bifida is a disabling condition,
it is easy for an affected individual
to lead a sedentary, low quality life,
existence. There are ways of getting
a child with spina bifida to become
more physically active. The Spina Bifida
Association outlines a number of adaptations
that can be made to allow participation
and competition in common activities.
Some of the items listed include making
the game ball larger or smaller according
to the activity being conducted, lowering
the net or goal, and tethering a ball
to a wheelchair using an elastic band.
Equipment modifications are not the
only method of encouraging participation,
field dimensions can be altered also.
Soccer goals can be wider, service lines
can be closer to the net, and making
the field larger or smaller gives a
child with the disability equality on
the field.
Along with equipment and field adjustments,
rules can be modified to implement equality.
This can range from altering the amount
of people on a team to creating a pass
rule where everyone must touch the ball
before a point can be scored. Sandler
(2004) suggests that there should
also be a connection between the child's
physical therapist and the teacher responsible
for PE at the school. Together they
can work in the best interest of the
child and create plans to integrate
the child into all aspects of the class'
physical activities. All of the aforementioned
modifications are pivotal in allowing
disabled individuals of all types to
interact with classmates, develop confidence,
and improve motor skills. Thanks to
the Individuals with Disabilities Education
Act (IDEA; Public
Law 101.476), this type of implementation
is now mandated to ensure equality for
all students (Spina
Bifida Association).
A technique vital to people with spina
bifida, who use wheelchairs, is enhancing
short-sitting balance. Dynamic short-sitting
is a commonly used tool in therapy that
aids in improved balance to decrease
fall rates, prevent further spinal damage,
and increase physical vitality. This
type of therapy is vital, but patients
only benefit as much as the effort they
put in. Dynamic sitting exercises contain
minor repetitive movements that help
with posture. The problem is that patients
are not motivated in any way to complete
these exercises, and are likely to neglect
its significance.
Researchers at the University of Manitoba
tried to tackle this issue by utilizing
an uncommon yet extremely effective
adaptation to combat the flailing interest
in dynamic short-sitting exercises.
They have created a video game program
that employs an incentive-based objective
to enthuse the patients and motivate
them to complete the exercise. This
is a clever solution, because it allows
for a more complete and effective treatment.
This system can be used for patients
other than those with spina bifida.
A experiment involved three men who
relied on a wheelchair for primary mobility.
The first patient was a 52-year old
man with complete paraplegia affecting
T11 – L1, and a transformational
amputation; both resulting from a motor
vehicle accident. The second patient
was 43, and suffered from a severe traumatic
brain injury. As a result he endures
poor lower-extremity muscle control
and high muscle tone. He had no sensory
loss, but was unable to maintain short-sitting
balance. The final patient was a 26
year-old man suffering from severe spina
bifida (myelomeningocele). His condition
extended from T10 to L2, giving him
complete paraplegia and poorly developed
lower extremities.
Most people take the ability to maintain
balance for granted. The report by Betkar
et al (2007)
gives an adequate definition of human
balance: "Balance of the human
body requires timely control of the
position and motion of the center of
body mass relative to the base of support."
Maintaining balance in a short-sitting
position requires the collaborated use
of many sensory and motor processes.
The great part about the video game
system, which is referred to as a COP-video
game (Center of Pressure), is that is
creates a virtual reality that takes
this definition of balance, and all
the factors that make it work, and incorporates
them into a fun game for patients to
use.
An example is the Balloon Burst
game. The patient is placed on the edge
of a table on a mat that can detect
position and weight distribution. Balloons
will appear at varied positions on the
screen. When a balloon pops up on the
left side of the screen the patient
will shift his weight to the left while
maintaining balance in order to pop
the balloon. Other game titles include
Under Pressure and Memory
Match. The beautiful thing about
the game is that its settings can be
modified to suit the progress of the
patient. The balloons can be set to
appear in a variety of directions, to
become smaller targets, or even appear
at a faster rate allowing for quicker
movements. This is to keep the person
interested in the game and to gradually
increase the difficulty. Also, the sensitivity
of the mat can be altered so that the
severely disabled can participant and
still be competitive (Betkar
et al, 2007).
Obviously the results of this study
are outstanding. Each of the three men
that participated exhibited notable
decreases in fall rates. Its effectiveness
is good news because the system is cost-effective
and portable, so it is able to reach
a plethora of therapy centers and even
conveniently act as an in-home system
(Betkar et al,
2007).
Possibly the greatest gift a parent
can give to any child of any form is
love and reassurance. This is especially
essential to a young child dealing with
spina bifida. Science Letter
(2006) describes a young eight
year old-girl by the name of Linnea
who at one point in her life was baffled
and disappointed with the way she entered
this world physically. This despondency
was mainly derived with her own comparison
between her and her school mates. Her
mother stated that around the age of
four and a half she began to realize
she was different from others. She cried
frequently because she was sad she was
born "with a hole in her back."
The article is ultimately about how
this young girl has grown to accept
her state and think of herself as an
equal among her peers. Her mother's
response to her tears is one of the
reasons the article has an uplifting
end:
"I told her that I was sad too, but that I loved her and was glad that she was my daughter. I told her that being sad did not change anything; she still had to take her medicine or have surgery because life goes on."
It is this kind of devotion and encouragement
that is imperative for a child that
is overwhelmed by the heartbreaking
feeling of being different from others.
It is imperative because it affects
many aspects of a child's life in a
positive way. At six weeks old the mother
was told that her daughter would never
roll-over, sit-up, crawl, or walk. At
age five, Linnea underwent tethered
spinal cord surgery and with the help
of her ankle foot orthotics she is active
in her physical exercise class and has
gained the respect of her classmates.
She explained to her classmates what
spina bifida is, and in response was
told by her peers that she wasn't thought
of differently. Without her mother's
optimistic view of her child's position
she would have never received the proper
medical care, the necessary adaptations,
and most importantly, the confidence
she uses to excel socially.
Spina bifida, with adequate knowledge
and adaptation, can be transformed from
a permanently disabling disorder to
a mere minor inconvenience when the
proper measures are taken. These proper
measures can be in the form of allowing
a child to practice serving aces from
the service line instead of the baseline
on a tennis court; it can be playing
an interactive video game in the comfort
of a home; and it can simple be a couple
words of encouragement from a classmate
or a parent. Whatever the measure, the
word equality should be on the mind,
and affection in the heart, so that
actions reverberate to others and make
in impact not just to the child with
spina bifida, but also to the peers
around the child.
Works Cited
Adrian Sandler
2004. Living
with Spina Bifida. UNC press, p.156.
Betker, Aimee
L; Desai, Ankur; Nett, Cristabel; Kapadia,
Naaz; Szturm, Tony
2007.
Game-based Exercises for Dynamic Short-Sitting
Balance Rehabilitation. Physical Therapy.
56(87): p. 1389.
Informational
Article
2004. Neural
Tube Defects. Complete Home Medical
Guide.
Journal Article
2006. Spina
Bifida; Special 8-year-old girl demonstrates
how to live with spina bifida. Science
Letter, p.1349.
Newsome, Brian
2007. Hope for
Parents born with Spina Bifida. Tribune
News Service, p.12.
Powerpoint Presentation
Adapted PE for Youth with Spina Bifida.
Spina Bifida Association.
|

